For a long time, the field of autoinflammation has been almost entirely dominated by the “three classic inflammatory factors” — IL-1β, IL-6, and TNF-α. Most mechanistic studies, target development, and clinical diagnosis and treatment have revolved around these traditional pro-inflammatory factors.
The core reason for focusing on these three factors is very clear: the inflammatory phenotypes they induce are the most intuitive, the signaling pathways are the clearest, and clinical validation is the most convenient. IL-1β and TNF-α can directly trigger high fever, redness, swelling, pain, and acute-phase responses (elevated CRP and ESR), and they are located downstream of the inflammasome, making their signaling pathways straightforward and easy to understand. In addition, the early clinical success of IL-1 inhibitors and TNF antagonists further reinforced the established perception that “autoinflammation is equivalent to traditional inflammatory factor-mediated inflammation.”
In contrast, the interferon axis centered on IFN-γ was neglected for a long time. Although interferons are also inflammatory factors, their mode of action is more concealed. They are mainly secreted by NK/CD8+ T cells and do not directly induce typical acute high fever. Therefore, they were categorized into antiviral immunity and autoimmune research rather than being regarded as a core regulatory pathway in autoinflammation.
Clinical Dilemmas Driving a Paradigm Shift: Why Traditional Treatments Frequently Fail
Breakthroughs in paradigms are often driven by clinical dilemmas. Classical autoinflammatory diseases represented by mevalonate kinase deficiency (MKD) have long been classified as inflammasome diseases driven by IL-1β, with IL-1 inhibitors being the first-line clinical treatment. However, in reality, a large number of patients respond poorly to traditional therapies, and severe cases can rapidly progress to HLH/MAS-like inflammatory crises. This indicates that traditional inflammatory factors may not be the core drivers of such diseases.
Disruptive Discovery: The Real Culprit in MKD Is the IFN-γ Storm
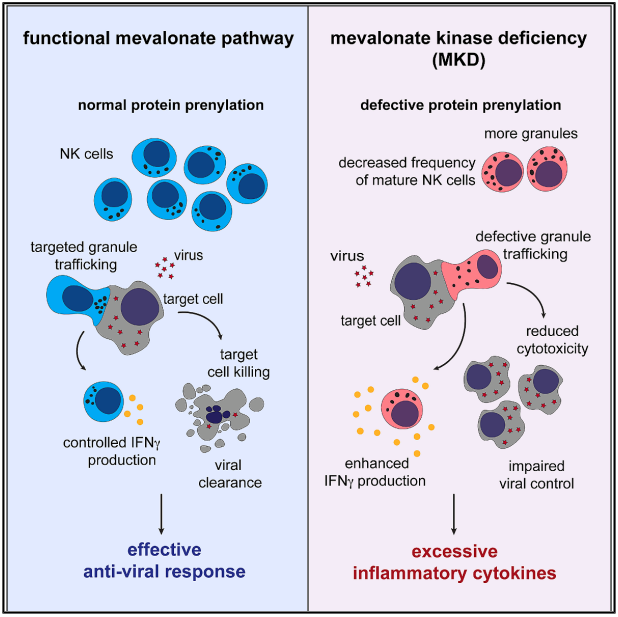
A recent study published in Immunity broke this cognitive deadlock and proposed a disruptive conclusion: the core pathogenic mechanism of MKD is an IFN-γ storm triggered by NK cell cytotoxicity defects.
MVK mutations lead to abnormalities in the mevalonate pathway, resulting in defects in protein isoprenylation, which in turn cause impaired NK cell maturation and abnormalities in cytotoxic granule transport and polarization. This produces an imbalanced phenotype characterized by reduced killing function but abnormally excessive IFN-γ secretion. At the same time, CD8+ T cells also exhibit similar functional defects, preventing the body from effectively clearing viruses. Persistent immune activation further amplifies IFN-γ release, ultimately triggering uncontrolled systemic severe inflammation.
This mechanism explains the fundamental reason why traditional IL-1-targeted therapies are ineffective and also pushes the interferon axis to the core position in autoinflammation research.
Original link:https://www.cell.com/immunity/fulltext/S1074-7613(26)00138-X
Why Can the Interferon Axis Become a New Research Track?
The interferon axis has rapidly become a research hotspot because it possesses broader applicability and greater clinical translational value than traditional inflammatory factors:
1. Broader clinical coverage: Abnormal IFN-γ signaling is involved in high-risk scenarios such as fever of unknown origin, refractory inflammation, infection/vaccine-triggered flare-ups, and MAS/HLH.
2. Higher mechanistic hierarchy: It deeply links metabolism-immune crosstalk, cytotoxic immunity, and the JAK-STAT network, serving as a key hub connecting immunodeficiency and severe inflammation.
3. Clear translational pathway: JAK inhibitors can directly block downstream signaling, rapidly achieving a closed loop from mechanism to treatment.
4. Huge innovation space: It avoids the overcrowded competition surrounding IL-1β/NLRP3 and opens new research directions.
Shifting Toward a New Direction: The Interferon Axis Opens a New Research Landscape
By shifting toward the interferon axis, researchers no longer need to remain limited to highly crowded mature targets such as NLRP3 and IL-1β. Instead, they can focus on directions including NK/CD8+ T-cell cytotoxicity, protein isoprenylation, small G protein regulation, and interferon downstream chemokine networks.
As the research space surrounding traditional inflammatory factors gradually narrows, the interferon axis centered on IFN-γ is becoming one of the next major hotspots in the field of autoinflammation due to its more upstream regulatory role, more critical contribution to severe inflammation, and clearer translational pathway.
Relevant indicators of Reed Biotech
|
Cat.No. |
Product Name |
Sample Amount |
|
RE1059H |
Human IFN-γ(Interferon Gamma) ELISA Kit |
100μL |
|
RE1059HF |
MF-Human IFN-γ(Interferon Gamma) ELISA Kit |
25μL |
|
RE1059M |
Mouse IFN-γ(Interferon Gamma) ELISA Kit |
100μL |
|
RE1059MF |
MF-Mouse IFN-γ(Interferon Gamma) ELISA Kit |
25μL |
|
RE3405M |
Mouse IFN-γ R1(Interferon Gamma Receptor 1) ELISA Kit |
100μL |
|
RE1059R |
Rat IFN-γ(Interferon Gamma) ELISA Kit |
100μL |
|
RE1059RF |
MF-Rat IFN-γ(Interferon Gamma) ELISA Kit |
25μL |